
A child born in a Glasgow, Scotland suburb can expect a life 28 years shorter than another living only 13 kilometres away. A girl in Lesotho is likely to live 42 years less than another in Japan. In Sweden, the risk of a woman dying during pregnancy and childbirth is 1 in 17 400; in Afghanistan, the odds are 1 in 8. Biology does not explain any of this. Instead, the differences between – and within – countries result from the social environment where people are born, live, grow, work and age.
This is a quote from the recent report from the WHO’s Commission on Social Determinants of Health. It is a fascinating document of worldwide health inequalites, and vividly details how such unfair differences can occur within countries and even within small populations. This issue is what I was discussing on my recent post on health inequalities in Beijing. Those of you interested in learning more about this topic should definitely read the above report, as well as some outstanding resources from other public health groups which can help you learn more about the concepts of health inequality and a social gradient of health.
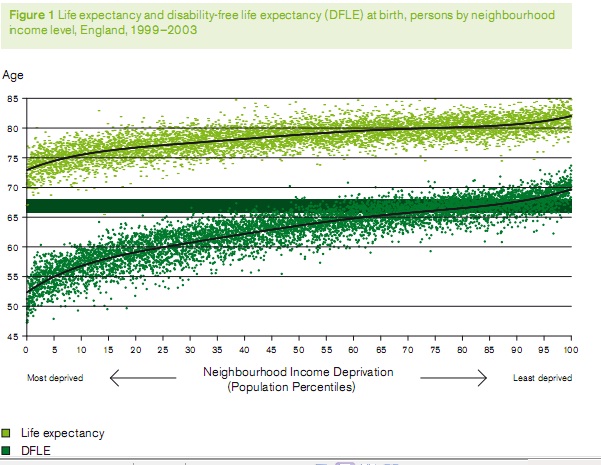
Those of you from the UK should definitely read the February 2010 Marmot Review, which details in very readable language how even in an advanced first-world economy like the UK, there are still large differences in health between different social groups. Subtitled “Fair Society, Healthy Lives”, it lucidly reviews the evidence showing concepts like the social gradient — how lower income levels have lower life expectancy and more disability:
One of the more concerning findings in both reports is that childhood and pregnancy factors play a large role in that child’s future health as an adult. For example, the most premature babies have a higher risk of diabetes and heart disease as adults:

Here’s a troubling graph below from the Marmot report showing how lower IQ children, when living in a higher socioeconomic neighborhood, can almost catch up to higher IQ children, while those in poorer neighborhoods continue to lag behind:

It is dramatic data like this which drives the WHO and other policy makers to encourage much more intervention of improving not only access to healthcare but improving neighborhoods, job satisfaction, and inequalities of poverty.
The Bottom Line?
For me, now that I know all this, I may be much more thorough asking about history and social issues in physical exams. For example, if I screen a 40-year old man who has great labs but then tells me he was born “a premie”, then I may be advising him more about diabetes risks and how he can help, and I may check his sugar levels more often.
I suppose all of this “new” research is simply a modern extension of holistic medicine…
Follow me on Facebook: @BainbridgeBabaDoc
Photography: www.richardsaintcyr.com
Low birth weight babies are much more at risk of being fed formula. I don't know if there are any papers about adding "just a little" formula. But formula feeding (as opposed to breastfeeding exclusively) has also been definitively linked to diabetes.
About "just a little" formula, I once read that the criteria for being considered in the "breastfed baby" category for a study, a baby can receive, at maximum, ONE eight- ounce bottle per every two weeks. It seems that the formula even occasionally ingested affects the gut flora so negatively, and the overall health, that they have strict definitions of the amount of formula a baby can have, and still be considered "breastfed".
Just a thought about the birth weight and diabetes chart. Very interesting.
And congratulations! I'd be willing to take a survey, and spread the word.
Here's an email from a reader:
"…Hi Dr. Saint Cyr,
I've been reading your blog about healthcare in Beijing and was
interested in what you wrote about
healthcare disparities among ex-pats in Beijing.
A friend of mine who was working in Beijing without the support of a
foreign-based institution did so without insurance for the year. She
was healthy for much of the year, but towards the end developed a
vaginal infection that she assumed was a yeast infection. She made an
appointment with an ex-pat clinic, but due to the cost and hoping the
infection would clear, decided to cancel the appointment. Instead she
tried to find treatment on her own at local pharmacies. The
pharmacists did not understand her Chinese translation of 'yeast' and
after purchasing three or four products that didn't clear the
infection she eventually found a more medical translation and
purchased a product that cleared the infection.
I've met several other people who are working in Beijing
independently, but we've never explicitly
talked about healthcare. My guess is many would delay care or
self-treat instead of visiting an
expensive ex-pat clinic.
Your project sounds very interesting, but I think it will be difficult
to get a representative sample of ex-pats in Beijing…"